
Helping Professionals Understand Childhood: A Work in Process
Part 2—The Educational Value of Supervision with Videos
Nathaniel Donson
Nathaniel Donson, M.D., an analyst-psychiatrist, is a psychiatric consultant at the Youth Consultation Service Institute for Infant and Preschool Mental Health in East Orange, New Jersey. He is a faculty member of Columbia Psychoanalytic Center for Training and Research.

Nathaniel Donson
In the last issue, TAP 51/4, we described the comprehensive multi-pronged model of the developing mind utilized at the Youth Consultation Service Institute for Infant and Preschool Mental Health, a nonprofit training and clinical facility caring yearly for about 300 families and their children in an innercity location near Newark, New Jersey. We outlined a case conference format designed to enhance students’ understanding of a psychoanalytic model of the mind that includes three important themes: developmental, psychodynamic and dyadic (or relational).
In this issue, we describe our procedures in further detail, which we hope others may utilize, as well as suggest alternate perspectives. Importantly, since psychoanalysts are usually uncomfortable videotaping their own sessions (even with consent of the patient) or supervising videotaped sessions, we will welcome your thoughts on the supervision of videotaped psychotherapy sessions.
Our supervisory process includes two sessions: First, a written text is discussed by students and faculty. This is followed a week later by presentation of a video that always includes the therapist.
As a guide to understanding the child’s history, we use a “timeline” as a visual metaphor for understanding concepts of developmental progression and regression, indicating critical periods when developmental tasks may be disrupted by inner or outer stresses. Atop the line are the usual sequences of intrapsychic maternal and child tasks, considered along a number of developmental lines, which (for example) may include: the gradual accomplishment of parent/child motor reciprocity and contingency within an emotionally rich interplay; the parent and child’s capacity to participate in parallel processes of soothing in the face of distress; the mother’s and father’s capacity to move along in their own development in concert with the child’s emerging mastery of ego and defense mechanisms; the child’s many necessary steps toward a security of attachment via sufficient internalizations that will stabilize his individualization, autonomy and capacity for separations over the first few years. Here a number of differing developmental models may be employed. (In the diagram below, such developmental tasks are represented by *’s)
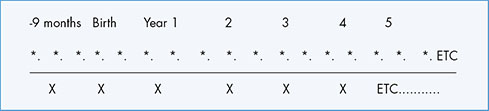
Below the line are stressful events (X) which may be unique or recurrent, showing diagrammatically what phasic ego tasks may be in process when they occurred. Often they may be multiple, unknown or variable.
Our students keep in mind that stress is not necessarily traumatic. (See Erna Furman’s “When Is the Death of a Parent Traumatic?”) If there was a single event (e.g., parental loss, medical illness, injury, fire in the home), how did the family respond? When and how did regressions to earlier modes occur? What was the course of the child’s recovery? If a single episode of abuse or neglect is known, were there others? And too often we also need to wonder whether the family is hiding some secret event or forbidding their child from knowing something.
Using Videos in Supervision
Our model of supervision (incorporating a relational theory of the mind) focuses on the understanding of transference/countertransference enactments. Watching the videos, we pay particular attention to patient/therapist enactments and ask about the therapist’s inner experiences while doing the video. Our discussions always emphasize reciprocities in the experiences of both patient and therapist as we try to learn about the patient from the experience of the therapist.
We emphasize the differences between motor milestones and developmental milestones—the latter a mastery of internal, emotional and mental capacities that derive from internalizations of narratives in the earliest dyadic experiences—including the mastery of delay, self-regulation, contingent and reciprocal relational interplay with others, and resilient persistence at a task with confident efforts in the face of disappointment and failure. We discuss impulse and inhibition, conflict and conflict resolution, defense organization and character formation, the uses of regression and other defenses in the service of the ego, transference-countertransference enactments, and focus particularly on the child’s internalized relational narratives. Our goal is to help students understand that it is helpful in their work to interest themselves in the interior lives of children and their parents and, very important, to reflect on their own internal world.
In addition to discussing the family’s and child’s responses in setting up and participating in a video, we ask the therapist a series of questions:
Vignettes from Video
The following three vignettes illustrate what may happen during the video portion of case presentations, as our group discussions illustrate the value of viewing and discussing videotaped material. Often, what is observed in the videotape would not have appeared in supervision through process notes.
1. During a conversation between a therapist and mother, a 10-month-old toddler with a pacifier in her mouth first cruised toward the therapist, placing her hand on her knee. Both mom and therapist were intently focused on mom’s distress about her other children. The therapist and mother continued to converse but neither responded to the child. When the toddler then climbed a bookshelf and tried to pull off an item, mom took her by her arms and gently moved her to the floor. The toddler then made loud noises with a toy, wanting to become part of the conversation. When mom took the toy away, she calmly went to play in another part of the room, showing a bland facial expression.
Often, material observed in a videotape would not have been discovered in supervision through process notes.
Although the toddler made several gentle overtures to engage, mostly toward the therapist, she persisted only briefly. Climbing the shelf, then banging on a noisy toy, seemed an energized, but futile persistence of her frustrated wish to engage her mother. She is regarded by the staff as an “adorable” child. In our prior discussion of the therapist’s written narrative, we had wondered, whether for this mother, this baby might be “Another Baby, Another Chance,” Selma Fraiberg’s term for enhancing a mom’s reflective capacities with her newest child after she had failed with others.
We discussed this child’s evolving defense organization and nascent character structure, her apparent dissociative suppression of emotional responsiveness, her turning of assertiveness to passivity, her “altruistic surrender.” We felt perhaps her accommodating to limits without protest or persistence served to protect her relationship with a very fragile mother. The therapist’s non-responsiveness in the session, which mirrored the mother’s non-responsiveness, was discussed as an enactment, that is, an unconscious alliance with the mother’s attitudes toward her daughter. Perhaps in their next appointment, the therapist could observe and narrate what was happening. Although this mother could keep her daughter safe, we wondered whether showing her the video might help her to respond more contingently and empathically to her toddler. Her toddler had not yet given up.
2. J is a six-year-old who screams and occasionally scratches her face when she does not get her way, is afraid of loud noises, is always oppositional with toileting, and wets herself at night. Parents’ relationship was characterized by high levels of verbal and physical violence before their separation.
Her therapist (L) had described disliking her, and feeling emotionally distant and unimportant to J. Usually L felt far warmer toward children she worked with. She felt that J’s attachment to her did not feel specific to her, was perhaps indiscriminate, and occasionally hoped she would not show up for appointments. Although J pulled for engagement, and was often nurturing toward pretend play figures, L felt she was not nurturing toward her. However, at the end of every appointment J was reluctant to leave and hugged L many times.
In the video, to L’s surprise, her profound importance to J was dramatically evident. J was intensely tuned in, highly interested in L’s comments, and was often contingently reciprocal within their verbal interplay. She frequently stopped her play and regarded L intently when L tried to fix a play item or show J something.
J directed the therapist to take on various roles with human figures, sometimes as mother to child, occasionally switching to violent narratives. We wondered therefore what L’s feelings of distance might indicate about J. Reflecting on our own (viewers’) difficulties following J’s abruptly changing play, we could only guess at L’s difficulties following J’s internally conflicted narrative discontinuities, likely the impact of traumatic care throughout her earlier childhood.
J’s speech was rapid and intense, sometimes unintelligible. She fed her dolls, carried them around, then enacted violent fights between family members. After a romantic (sexual?) interplay between two figures, there was a fight; she repeatedly brought them to the roof of the dollhouse, then crashed them into the ground as her rhythms and prosody became louder, more intense and clearly full of excitement. We speculated about J’s affectively dysregulated emotional life. Perhaps she became anxiously manic and frightened by her excitement and sexual arousal. In another sequence, she disrobed one of the figures, again escalated her excitement, then dropped the figures from roof to the ground.
Here an uncomfortable countertransference can be useful diagnostically and therapeutically. By L’s discomforted participation in a parallel internal experience she had learned a lot about J’s emotional and mental life. However, by aligning her verbal rhythms and prosody with J’s play, we saw that L became a resonant responder to J’s dysregulated affective internal world. Her functioning as a more regulated container in her response had become a therapeutic “holding environment” (Winnicott), perhaps allowing J adequate emotional time and space to work through her traumatic interior life.
This video offered a vivid opportunity to explore J’s evolving defensive relational character structure, suggesting that an anxious post-traumatic profound emotional neediness was warded off by denial, reaction formation, affect reversals, and a powerful capacity for projective identification, insuring that L and not J would feel unimportant, unseen and overlooked.
3. Following immigration at age four to join his family’s father, at nine years X still resented the change, repeating endlessly that he wanted to go “home.” His mother felt the same way; both had difficulty learning English. It seemed this child’s interior world had remained in his country of origin as well as resonant with his mother’s state of mind.
In the video, we saw when X asked for help, he seemed not to want it, suggesting a conflicted internal (traumatic) narrative depicting “helpful” human encounters. The therapist (M) felt rejected by X, always uncertain about how to respond. M wondered why it was difficult for them to enter into a contingent and reciprocal interplay, although when X asked M about an item, M said, “I don’t know,” then put it back on the shelf. When X then requested M’s assistance to put on handcuffs, we wondered about his wanting restraint for his badness, perhaps as punishment. We pointed out these events as future opportunities to explore X’s feelings and thoughts.
X always played in a desultory and discontinuous fashion; every start was abruptly terminated. Perhaps traumatic memories had led to inhibitions of appropriate aggression and assertiveness, interfering with continuities in his play. However, we all felt that his interplay with M showed the beginnings of a bonding which in time would facilitate their work together.
At no time did X make eye contact with M. Yet, when the camera was moved he stared directly into it with a gaze that left some of us puzzled about what he saw or whether he avoided human faces. Poor vision had been picked up at three years; perhaps this visual impairment had disrupted his early maternal bonding.
M had tended toward limit setting in her therapy, aware that this was not being done well at home, but was uncertain whether to introduce more structure into the therapy. How else could M further her understanding of X’s mental life? I suggested she use Winnicott’s “Squiggle” game to introduce a partial drawing, or offer the beginning of a story to be handed back and forth to build a narrative. Such reciprocal play could help X more fully enter the relationship, as well as develop a vocabulary for affects and reveal more about his feelings. Hopefully he could internalize their interactions to help him establish sufficient reflective functioning, and ultimately engage in more secure play with other children.
X conveyed the impression to several of the viewers that he was “not aware of his body.” One observer commented that he “needed instruction” about appropriate dress. He had once said, “I don’t want to be grown up!” That observer, who had worked in a program for sexually abused children, worried that he would “go off with anyone” and become subject to sexual abuse.
Although none of us agreed, our custom in viewing videos is that no thought offered by a viewer is ever ignored. I once had the experience of asking students what they had seen in a video of a three-year-old girl. No one responded. After an uncomfortable silence, I told them I had fantasied her as a future pole dancer…. And three others admitted they had the same thought.
Some student follow-up comments: The first is a nearly universal response
Videos as Holograms
There are approximately 20 case conferences over the course of the academic year. Although we think of our videos as holograms, containing massive amounts of information, it invariably becomes clear that we are able to study only a small arc of a parent and child’s internal lives and narratives and to discover thereby only a few provisional therapeutic windows for the therapist to consider. Clearly, the video provides an additional supervisory richness that allows therapists and supervisors to observe a variety of interactions that would have been overlooked or “forgotten” and therefore not reported if supervision were done only with process notes.
The pedagogic effectiveness of this case conference model has not yet been systematically studied, but we have found that our students’ appreciation of the interior lives of their patients strengthens over the course of the academic year. Ultimately many of them emerge from their internship and externship year understanding and using developmental, psychodynamic and relational (dyadic) terminology within their therapeutic work, and expressing their appreciation for the usefulness of a theory of mind in enriching their clinical thinking.
From the Issues in Child and Adolescent Psychoanalysis Editor
In Part 2 of his article about a program designed to help professionals understand childhood, Nathaniel Donson, the psychiatric consultant at the Youth Consultation Service Institute for Infant and Preschool Mental Health in New Jersey, highlights a vital aspect of the process that may enrich our own teaching and supervision.
The most important part of his contribution is Donson’s discussion of the value of reviewing videotaped psychotherapy sessions. For example, one therapist, before watching herself in a video, had not appreciated the depth of the child’s attachment to her. When watching the video, her importance to him was dramatically evident. She commented that it was helpful for her to see she was doing far more than she thought. Another student noticed in the video she had slipped into being with the child in ways that both parent and school wanted, but evoked opposition and frustration.
The use of videotaped supervision has become particularly important for me, as well. In our treatment trial of Regulation Focused Psychotherapy for Children (RFP-C) (https://www.rfp-c.com), all sessions are taped. Therapists participating in the study are all Psy.D. predoctoral students, similar to the educational level of those working with Donson. Both therapists and supervisors have always found video supervision to be valuable.
In TAP 52/2, members of our team will write about our work.
—Leon Hoffman
Editor’s Note:
Readers interested in finding out more about the comprehensive multi-pronged model of the developing mind are welcome to contact the author at MNDonson@aol.com, his office 201-568-5217, or cell phone 201-835-9969.