
Annie Lee Jones
SPECIAL SECTION: CONVERSATIONS ON PSYCHOANALYSIS AND RACE
Annie Lee Jones
Annie Lee Jones, Ph.D., is a clinical psychologist/psychoanalyst in private practice in Queens, New York, and a co-chair of the Committee on Ethnicity, Race, Culture, Class and Language (CERCCL) at the New York University Postdoctoral Program in Psychotherapy and Psychoanalysis.
Annie Lee Jones
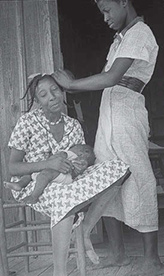
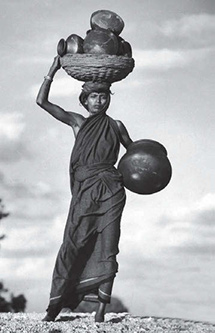
Over the years I have learned that the photos of African-American women on the walls of my office have become an integral part of who I am perceived to be by my patients. Some of the photos are of elderly former sharecroppers, poor women straightening their own or another’s hair with hot combs, some are of nomadic women carrying vessels on their hips or heads.
My patients told me the photos have served as a kind of bridge to spaces in our work that are safe for them to wonder about me as their analyst. Additionally, patients have offered thoughts about what each photo represents to them based on their own backgrounds. It is through the use of me and my photos that we begin to formulate previously unarticulated psychodynamics and historical narratives.
Some have also said they notice aspects of me reflected in the photos during silent reveries in their sessions. Sometimes during the initial interviews patients ask me direct questions about the photos and share their associations along with their thoughts on why they selected me to begin treatment. The freedom to explore their perceptions of me in my office during the early stages of our work has proven to be very important to the treatment process. Some patients, while making note of the fact that I practice in their neighborhood will wonder out loud if I live nearby. Others will ask me about my own ethnic origin within the African-American diaspora.
Shared encounters like these can quickly lead to transference and countertransference processes centered on mutually recognized experiences. These shared encounters offer opportunities for exploration of the patient’s introduction of recent life events that on the surface do not appear to be related to what has gone before, but can lead to the resurfacing of losses attached to their mourning process.

The patient’s musings about the possibilities of their analyst’s daily life can trigger some shared relational links to media-driven experiences of fear-inducing events that appear to be typical in the everyday lives of those who live and work in our community. Loss-grief, shame-embarrassment, and fear of repetition become shared in complex ways between patient and analyst as the patient tells the analyst who she is and where she came from. Many find the initial “taking of the developmental history” traumatic.
Impact of Lost Family History
It is not uncommon for the patient to starkly inform the analyst that she does not know anything about her grandparents, for example. Some patients struggle to describe the feelings associated with paternal or maternal absences. War, migration, social upheavals, economic distress and other forces have a tremendous impact on the personal histories of many of my patients. In most cases, they identify racial discrimination, caste and class-driven violence, along with poverty, as the cultural forces responsible for the major disruptions in their genealogy. It is common for them to announce it grieves them deeply that they do not know their family history at the very point in their lives where they are poised to work in psychotherapy to get to know better the self they are.
The psychoanalytic dyad of two African-American women can offer possibilities for empathic recognition that facilitates treatment. The dyad and its mutually constructed dynamic can be informed by many factors not usually a component of psychoanalytic discourse around theory and training. The race-based and ethnically informed relational exchanges that shape the work are yet to be incorporated in contemporary psychoanalysis. Over the years, Megan Obourn and I, as well as others, have written about the way culturally informed racialized object relations work in everyday life.
Benjamin Wolstein (1994) points to the relevance of these observations when he states that “clinical involvement with the larger social and cultural environment in which the therapist and patients live out their daily lives was considered novel” and that intrapsychic phenomena do not exist in a vacuum—they occur in the context of “extrapsychic phenomena.”
I have written elsewhere (Jones and Obourn, 2014) about my understanding of how hatred and fear directed at the blackened object have historical, political, economic, cultural and social implications for how our internal world is constructed. The legacy of chattel slavery is foundational and informs our group and individual psychodynamics. When current events reflecting injustice and inequality are brought into the session, our dyad’s experiences of these events can be effectively utilized both to provide a space where such events can be metabolized and a space where the potential for replication of oppressive experiences can be reflected upon rather than acted out in self-destructive ways. In this conceptualization of our work, I can facilitate the patient’s recognition that the larger social domain impacts the dyad’s individual psychologies. In so doing, I affirm my patient’s right to observe; such affirmation can soften resistances and open pathways towards illumination of internal conflicts requiring more in-depth exploration. As Earl Hopper (2003) suggests, we live in a traumatogenic society that can be relationally explored.
When a patient in an intense prolonged grief reaction gains a respect for the realities she has experienced, she can begin to consider altering her object relations to the lost loved one as Freud suggested in 1917. In doing this, the patient begins to recognize pathways to understanding the aspects of her mourning process that stay linked to the loss, and prolong the existence of the lost object’s influence on much of her everyday life. Her loss lingers over narratives created in the dyad. When recognized by the dyad, she can use this new experience to explore shared and evolving awareness of affective links to past traumas. I have found Donald Spence (1994) and Donnel Stern (1997) helpful in understanding narration and consensual validation.
As a person who began her training as a clinical psychologist and psychoanalyst in the Deep South during the heat of the Civil Rights Movement, it became important to me to create a treatment space where I could stabilize my own subjectivity as a psychoanalyst who is also an African-American woman. I am fully aware of many of the forms of gendered racism that inform my everyday experiences. My patients often report that their outlook for the future is complicated by fears of loss and grief. As Claudia Rankine so profoundly put it, “the condition of black life is one of mourning…. Mourning lived in real time.” Further, Rankine says (2015), “there is really no mode of empathy that can replicate the daily strain of knowing that as a black person you can be killed for simply being black.”
Some recent immigrants who enter treatment describe a loss of hope when they realize they cannot avoid the plague of American racism based on skin color. Some have detailed the broad spectrums of skin color variances that were typical of households in their countries of origin. Even after including skin color associations in their treatment, they seem to dissociate their experiences in the United States from similar experiences they had back home. It is my impression that their encounters with U.S. prejudice based on skin color are uniquely traumatizing.
Fresh Acts of Violence
News of acts of violence against African-Americans by the authorities or by other citizens are brought into the session with dysphoric affective links to their own lived lives.
Tayari Jones (2015) provides us with an example of this in her short piece called The Lingering Memory of Dead Boys:
Like many Americans, I have been glued to the television eager for details about the tragic murder of 17-year-old Trayvon Martin. I am not sure what I hoped to discover, as each new piece of evidence is more disturbing than the last. I listened to the recently released 911 tapes on my office computer and cried in public. I was up until after midnight scanning my Twitter feed for news and comfort, a twenty-first century vigil of sorts…. Learning about death and dying is part of growing up. If we are lucky, we come to understand that death is natural through the passing of a grandparent or some other elder. If we are lucky, we will be taught something about a life well lived. But for too many of us, we are made aware of our own mortality seeing our peers—the boys we want to go to the movies with, the boys who used to pull our hair—we learned that they could be killed for the crime [of] being themselves. Young. Black. And Male.
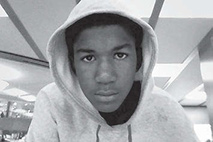
Along with many of my patients, I followed the unfolding of the details of the Zimmerman case after he killed Trayvon Martin. My patients report they found themselves crying out loud or weeping softly during each news update. During the immediate aftermath of the murder, some patients reported spending innumerable hours following Twitter feeds and other social media updates. While others dedicated large portions of their sessions to their experience of this material, some seemed to avoid detailing the daily news in their sessions and instead introduced dangerous encounters from their own childhoods. There were patients who also focused on their thoughts and feelings about their own mortality, which they related to the loss they imagined the mother of this child was enduring.
Those patients who reported feeling that their days were saturated with news of this tragedy also seemed to be those who found pathways back to formerly unarticulated losses of their own. Some patients started to explore how they first encountered death and dying as children. These patients seemed to also return to the ways their unique mourning process had been eclipsed, interrupted or stalled by current traumas in their own lives.
Patients also use the tragic death of Sandra Bland in police custody—referred to as “the Sandra Bland situation”—as shorthand for anticipatory fear that they relate to random encounters with law enforcement agents while traveling alone on the streets of their own neighborhoods. It may be that the co-creation of potential spaces in the treatment that allow for these types of associative explorations via the media offer the added benefit of reducing the personal negative impact of racial discrimination. This allows the patient room to reflect on and symbolize the pain of these experiences, rather than burying such pain or dissociating from it. She can then be freed up to turn back to what brought her to treatment.
Detailing the rash of media reports of violence and destruction of blackened bodies serves as a pathway to the individual’s unresolved grief and mourning, processes that have sometimes been transmitted across generations in the patient’s family. The legacies of repetitive losses are often encapsulated in individualized, developmentally charged expressions of the ways in which chattel slavery, caste systems and generational losses could not be contained by the patient’s family, or that the patient could not locate in prior relational spaces. Sometimes, black and dark skin associations mark each member of the dyad as participant, observer and/or witness. The dyad can thus become/create a containing relational space.
It seems that as patients chronicled fears of racial animus that infused their daily lives, they became more able to identify personal aspects of their developmental history that may have inhibited the mourning of past losses.
Fear of Police
Fear of random violence at the hands of the police is shared by many of my patients. As a psychoanalyst I have shared their terror as they recount experiences of contact with police and security guards. The patients’ attempts to figure out ways to feel more secure in their homes and neighborhoods and to develop strategies to avoid contact with the police when they travel outside their neighborhoods to work can be fraught with difficulty. They often couple their descriptions of these efforts with how they struggle to explain to their children the reality of their lives lived in black skin in America.
The ordinary everyday lives of black women in America can be plagued by the repetition of difficult to metabolize thoughts and feelings that can initially present as mild clinical states. Financially successful black women living and working in urban areas describe how they cope with being seen through the mist of poverty. They describe how the experiences of the poor are mapped upon them when they move around their world. They report feeling socially and politically isolated from urban centers of power and opportunity.
When some women described family members’ experiences with the policing tactic of Stop/Search/Question/Frisk, what they seem to fear most is finding themselves in the presence of such phenomena, and being caught off guard. They describe their fear of witnessing such police action, and they often indicate they equate such experiences with other types of community-based violence.
I have found the intergenerational transmission of unconscious memories linked to trauma and loss are never dissociated; instead they remain actively available in the reflective realm of the unconscious. A patient reported to me that whenever she is driving alone on her usual route to work, any news dispatches describing the shooting of a child, similar to the killing of the 12-year-old boy in Cleveland, induce her to become so overwhelmed with tears and breathlessness that she has to pull over immediately, blinded by her tears. Her description of the depth of her pain mirrors her description of discovering her mother dead in their family home when she was a child.
My work with patients often includes oral histories of ancestral enslavement, menial field work due to caste systems, as well as descriptions of heavy, (and often) dangerous underpaid factory work. Having finally made it to America, many people, paradoxically, begin to find the freedom to lament the limitations on their lives. They explore the effects of a prolonged generalized sense of anxiety and remorse over the risk of sudden loss they had experienced. Their fears seem to link to fantasies of loss at the behest of unknown others.
The immediate transmission of threats and acts of violence against black Americans via all forms of social media, television and news outlets underscores the risks that these acts can seem normative.
It is common that the isolation stemming from institutionally sanctioned segregated housing and schooling in major cities in the United States reifies dissociative processes around current losses and also reactivates the trauma of those losses that have gone before. This isolation and negation of the reality that African-Americans experience forecloses the opportunity to experience a general sense of freedom to be oneself, including the opportunity to communicate the fear of past and present loss. In this connection, the relational experience for many of my patients of having an African-American psychoanalyst serves as a validating relational affirmation that alleviates their isolation as they recall and metabolize these experiences. W. E. B. DuBois’s (1953) formulation of the double consciousness that African-Americans display as contrasted with a more authentic self is still a useful formulation to understand the unique relational possibility of shared validation for my patients in this dyadic experience.
The racial and ethnic undertones of the 2015-2016 campaign cycle are beginning to filter into some of my treatments. These undertones amplify the fears I have been describing above, and there is no resolution in sight. Many of my patients are mourning the loss of their ability to imagine life free of the risks they face simply because of how they are perceived by others. At the time of writing this article, the Chicago Police Department has just released a series of videos of the use of deadly force against its citizenry. I expect this news will surface in my practice next week, further complicating the relational dynamics of loss, grief and fear in our psychoanalytic processes.
Editor’s Note:
For more information about the sources in this article, you may contact the author at annieleejonesphd@gmail.com.